A few weeks ago, I ordered an anatomically correct female pelvis model for Humanaut Health. We use models like these to teach medical providers and medical staff about anatomy for exams, procedures, and treatments (like low-intensity shockwave therapy). It’s the kind of thing you want to get right because the whole point is accuracy. You’re teaching doctors and clinicians where things are so they can help real women with real bodies.
The model arrived. I unpacked it. I turned it over in my hands, inspected the bladder, the uterus, the vaginal canal, and the pelvic bone. It was nicely made. Detailed. Expensive. And it was missing something.
There was no clitoris.
I sat there holding this “anatomically correct” medical teaching model, designed to educate healthcare providers about the female pelvis, and the organ with the highest nerve density in the entire female body simply did not appear on it. The clitoris had been edited out. Deemed irrelevant to the practice of medicine.
And I thought: well, that explains a lot, doesn’t it?
It explains why many physicians can’t accurately describe clitoral anatomy. It explains why women are told their pain during sex is “normal.” It explains why dozens of women have come to my office and asked me, genuinely, whether their bodies were broken because sex was painful or orgasm elusive. They didn’t need new bodies. They needed someone to tell them the truth about the one they already had.
We wonder why women suffer in silence through painful sex, declining arousal, and disappearing orgasms without ever asking for help. They don’t ask because nobody ever gave them the right information in the first place. So let’s fix that. Right now. This is Part 1 of a three-part series called “Lies you were told about the Land Down Under.” Part 1 starts where the problem starts: with the map itself.
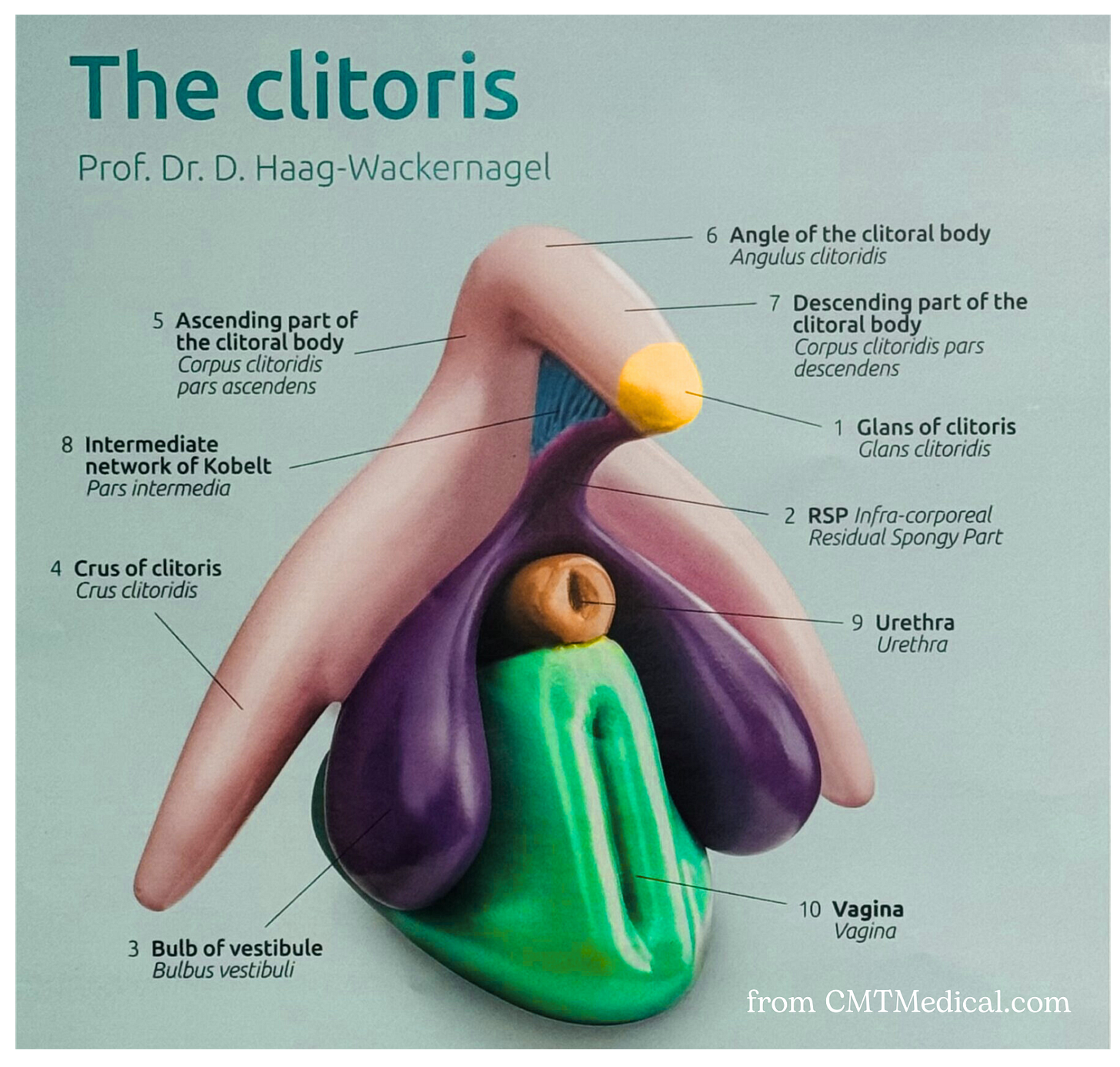
Lie #1: “The clitoris is a tiny button.”
This is the equivalent of looking at the tip of an iceberg and saying, “Oh, that’s a cute little ice cube.” The glans clitoris (the part you can see) is roughly the size of a pea. But the full clitoral complex, including the paired corpora cavernosa, crura, and vestibular bulbs, extends 3.5 to 4+ inches internally in a wishbone shape. It wraps around the vaginal canal and the urethra. It is composed of erectile tissue, just like a penis. When aroused, the internal structures engorge with blood, swell, and press against the vaginal walls. This is, by the way, the actual mechanism behind what people have been calling “vaginal orgasms” for the last century (more on that in Part 2).
How did we not know this? Because nobody bothered to look. Australian urologist Helen O’Connell published the first accurate, MRI-based anatomical description of the clitoris in 2005. Two thousand and five. We mapped the human genome in 2003, but didn’t get around to accurately describing an organ that exists in half the population until two years later. O’Connell herself noted that most anatomy textbooks were based on dissections of elderly cadavers whose erectile tissue had already atrophied. We were literally teaching medical students about the clitoris using bodies in which the clitoris had already shriveled up. You can’t make this stuff up.
Lie #2: “Your clitoris looks like my clitoris.”
It almost certainly does not. A 2024 meta‑analysis in Clinical Anatomy by Longhurst and colleagues pooled 21 studies and found substantial ranges in clitoral glans, body, crural, and bulb dimensions, as well as in the distance from the clitoris to the vaginal wall. Anatomical studies show that the paired vestibular bulbs, those cushions of erectile tissue that flank the vaginal canal, can occupy much of the space between the labia, clitoral body, and crura, with marked variation in their size and exact position from woman to woman. In practice, that means some women have considerably more internal erectile tissue hugging the vaginal wall than others.
Read that again. Some women have more erectile tissue surrounding their vaginal canal than others. This isn’t a lifestyle choice. It’s not about being “more sexual” or “less inhibited.” It’s anatomy. And it means that penetration is going to feel very different from one woman to the next, not because of technique or effort or the position of Jupiter in the third house, but because the underlying hardware is genuinely, measurably different. Your astrologer cannot help you here. Your anatomy textbook couldn’t either, but at least that’s fixable.
Nobody told you this. Nobody told your partner this. And that matters, because the myth that all women’s bodies work the same way has been weaponized against women who don’t respond the way a male-centered culture expects them to.
Lie #3: “The clitoris has 8,000 nerve endings.”
You’ve heard this number. It’s been floating around the internet, textbooks, and wellness blogs for decades. It came from livestock studies. Cows. We were estimating the nerve density of the human clitoris based on bovine research. Because why would we bother to actually count the nerves in a human one?
Well, in 2022, Dr. Blair Peters at Oregon Health & Science University finally did. His team obtained clitoral nerve tissue from seven volunteers undergoing gender-affirming surgery and, for the first time in history, counted the nerve fibers in the dorsal nerve of the human clitoris. The average? 10,281 fibers. That’s roughly 20% more than the cow-derived estimate. And since there are other nerves contributing beyond the dorsal nerve, the real total is even higher.
For context: the median nerve in your entire hand contains about 18,000 fibers. The clitoris is smaller than your thumb. Think about that concentration of sensation and then ask yourself why it took until 2022 for someone to bother counting. The cows had no comment.

Lie #4: “Your vagina is one size, like your arm.”
Your arm is always the same length. Your femur doesn’t grow two inches when you get excited about something. But your vagina? Your vagina is a shapeshifter.
In its resting state, the vaginal canal is about 2 to 4 inches long. The walls collapse against each other (it’s not a hallway, it’s a flattened tube) and are lined with folds called rugae that look and behave much like the folds of an accordion. When you’re not aroused, there’s not much room in there. A tampon fits. That’s about what the space is designed for at baseline.
But during arousal, something remarkable happens. Blood flows into the pelvic tissues, the rugae unfold and stretch, and the cervix and uterus pull upward and backward in a process called “vaginal tenting.” Masters and Johnson first described this in 1966 after observing over 10,000 sexual response cycles, and MRI studies have since confirmed it. The result? The vaginal canal can expand to 5 to 8 inches in both length and width. That’s roughly double its resting size. The tissue also changes color, deepening to a darker hue as blood engorges the walls, and the glands begin producing lubrication. Your vagina is, in essence, preparing itself to comfortably receive something it had no room for five minutes ago.
This is why foreplay is not a “nice to have.” It is a physiological requirement. If penetration happens before the vagina has had time to tent, you are trying to fit a 5-inch penis (or whatever he tells you it is) into a 3-inch space. That’s not a compatibility problem. That’s a timing problem. The discomfort she feels when sex happens too fast isn’t because something is wrong with her body. It’s because her body wasn’t given enough time to do what it was literally designed to do.

And here’s the part that matters for my midlife readers: estrogen plays a central role in maintaining the elasticity of those vaginal walls and the health of the rugae. As estrogen declines in perimenopause and menopause, the tissue thins, the rugae flatten, and the vagina’s ability to expand during arousal diminishes. This is one of the many reasons vaginal estrogen (or systemic estrogen, or both) isn’t a luxury for postmenopausal women. It’s what keeps the accordion working.
All (adult) vaginas need estrogen. If you’re not making it, take it. I’m gonna get a billboard with that on it someday.
In Summary…
So let’s recap. You have a complex, erectile organ with over 10,000 nerve fibers that nobody accurately described until you were old enough to have a mortgage. You have a vaginal canal that can double in size when properly motivated, but no one taught you (or your partner) that it needed a warm-up period. You have internal anatomy so variable from woman to woman that comparing notes with your best friend over wine is essentially useless, although I fully encourage you to do it anyway.
This is the foundation. The map of the territory. And I need you to have it before we go where we’re going next, because in Part 2, we’re talking about orgasms. Specifically, the lies you’ve been told about how they work, why you’re not having them, and who exactly decided that the sexual playbook should revolve around an organ you don’t have.
Spoiler: it was Freud. It’s always Freud.
P.S. I “fixed” the model pelvis with a black Sharpie and a sizable clitoris. If it’s going to be a DIY project, our plastic model woman deserves all the benefits I can give her. 🙂
P.P. S. If you want to learn more about what your clitoris thinks about things like testosterone therapy, vaginal estrogen, and the idea of shrinking with age, check out my interview with your diva down under in “Hi. It’s Me. Your Clitoris.”
This article was originally published on Dr. Amy Killen’s Substack newsletter. Subscribe for free to get new posts delivered to your inbox.
Are you a medical provider? Learn to prescribe hormone optimization therapy with the frameworks, protocols, and confidence you didn’t get in training.
Get Dr. Amy Killen’s Newsletter
Hormones, longevity, and regenerative medicine — straight talk from a physician who actually prescribes it. Free, weekly-ish, no spam.