Most women on hormone therapy are using estradiol completely correctly and also completely wrong at the same time.
They’re taking it. They’re consistent. They’re doing exactly what their doctor advised. But nobody told them about the small, evidence-based tweaks that could make a massive difference in how they actually feel.
Estradiol is powerful stuff. It affects your brain, bones, metabolism, sex life, cardiovascular system, and mood. It’s one of the most essential hormones in your body, and for women in perimenopause and beyond, it’s often the difference between feeling like yourself and feeling like you’re living in a house of mirrors that stopped being fun several years ago.
But how you use estradiol can matter almost as much as the fact that you’re using it.
Below are 11 surprising, science-backed estradiol tips and tricks. Some of them will seem counterintuitive. A few might contradict what you’ve been told. All of them are backed by data.
Let’s get into it.
1. Smallish Area = Better Absorption (for Gels)
This one shocks everyone, including doctors.
For alcohol-based estradiol gels such as Divigel or Sandrena, applying the gel to a smaller skin area yields better absorption and more stable estradiol levels than spreading it over a larger area. In one estradiol gel study, the best absorption happened at 200 – 400 cm(2) surface area (about the size of one to two human hands), whereas absorption was much lower when the gel was spread out further.
Wait, what? Doesn’t more surface area mean more absorption?
Nope. Here’s why: when you apply estradiol gel to a concentrated area, you create a stronger diffusion gradient. Think of it like the difference between dumping a bucket of water on a small patch of soil versus misting that same amount of water over your entire yard. The concentrated dose drives the hormone deeper into the skin more efficiently.
The practical takeaway here is simple: one forearm or a palm-sized spot on your inner thigh is perfect. You don’t need to paint your whole arm like you’re applying sunscreen before a beach day. In fact, spreading it too thin might be working against you.
This is one of those things that I was actually doing wrong with my patients until I read the pharmacokinetics studies and changed my tune. Oops!
2. For Creams, the Data Is Different (But the Logic Probably Isn’t)
If you’re using compounded estradiol cream instead of an alcohol-based gel, we don’t have the same level of research on the area versus absorption. The studies just haven’t been done with creams the way they have with gels.
But here’s what we know from basic skin pharmacology: the same principles likely apply. Thin skin plus a modest, concentrated area probably equals better absorption. Spreading one milliliter of cream over your entire torso like it’s body lotion? You’re probably diluting the concentration too much to be optimal.
The goal isn’t to be militantly precise about this. You’re not defusing a bomb. Just avoid the instinct to spread it everywhere. Keep it focused, keep it consistent, and your body will thank you.
3. Warm Skin = Better Absorption
Estradiol penetrates better through warm, well-perfused skin.
Blood flow matters. When your skin is warm, blood vessels dilate, circulation increases, and the hormone has an easier path into your systemic circulation. Cold, goosebumpy skin with vasoconstricted blood vessels? Not ideal for absorption.
The best bet here is to apply your estradiol after a warm shower or after you’ve been moving around a bit. Your skin doesn’t need to be hot, just comfortably warm and receptive. If you apply it after coming in from the cold, you won’t achieve optimal absorption.
It’s a tiny tweak that costs nothing and can genuinely improve how well your dose works.
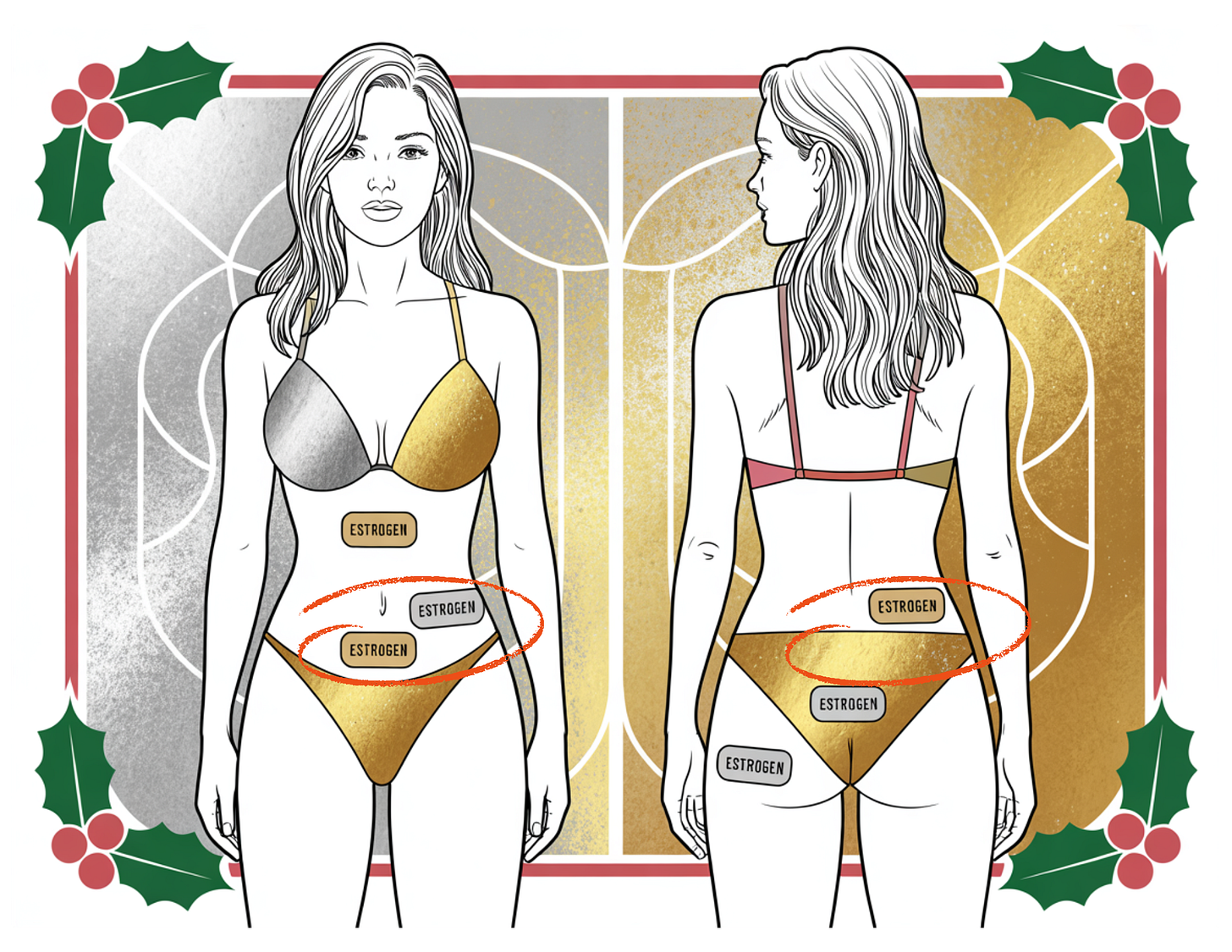
4. Where You Apply It Matters
Not all skin is created equal when it comes to hormone absorption. Some areas absorb estradiol beautifully. Others are unpredictable at best.
Here’s the breakdown:
Better absorption sites:
-
Inner forearms
-
Inner thighs
-
Lower abdomen
Less predictable:
-
Outer hip
-
Areas with thick subcutaneous fat
Avoid entirely:
-
Breasts (they’re super absorbent locally, which is exactly why we don’t use them for systemic dosing. You’ll get concentrated effects there rather than even distribution throughout your body)
The differences aren’t trivial. If you’ve been applying estradiol to your outer hip because it’s convenient and wondering why your symptoms aren’t improving, this might be why. Small site choices can genuinely change how you feel.
5. Patch Placement Is Not Random
If you’re using estradiol patches, they have favorite spots. This isn’t marketing copy. It’s based on absorption studies.
Patches work best when applied to the lower abdomen or upper buttocks. These areas give you more consistent, reliable estradiol levels. Thighs and hipbone areas? Less consistent absorption, more variability in your levels.
The recommendation to rotate sites is still valid. You don’t want to irritate the same patch of skin over and over. But rotate within the good zones. Don’t cycle through random spots on your body like you’re playing hormone roulette.
Consistency matters, and placement matters. Choose wisely.
6. Lotions, Oils, and Self-Tanner Can Interfere
Your estradiol needs a clean entry point. It’s trying to get through your skin barrier and into your bloodstream, and anything that creates an additional barrier or changes the skin’s permeability can interfere with that process.
Applying heavy lotions, body oils, sunscreen, or self-tanner under or immediately after your estradiol can alter absorption. Sometimes they block it. Sometimes they enhance it unpredictably. Either way, you’re introducing variables you don’t want.
The fix is straightforward: apply estradiol to clean, dry skin. Let it sit for 10 to 15 minutes before layering other products on top. If you have a complex morning skincare routine, factor in the brief waiting period. Your estradiol deserves to go on first, alone, without competition.
7. Vaginal Estrogen Can Raise Systemic Levels Slightly – and That’s Normal
This one freaks people out unnecessarily.
Even low-dose vaginal estrogen can temporarily nudge your blood estradiol levels upward as the vaginal tissue heals and starts absorbing better. This is especially common in the first few weeks of treatment when the tissue is most atrophied and then suddenly gets a hormone it’s been missing.
Is this dangerous? No. Is it “too much estrogen”? Also no. Is it a reason to panic or stop therapy? Absolutely not.
It’s just physiology doing its thing. As the vaginal tissue restores itself, absorption often normalizes. If your doctor sees your serum estradiol go from undetectable to 30 pg/mL after starting vaginal estrogen and acts like you’re overdosing, they’re overreacting. Context matters. Symptoms matter. This is not a crisis.
8. Oral Estradiol Isn’t “Bad” – It Just Has a Personality
You’ll often hear that oral estradiol is inferior to patches or gels, that it’s outdated, that transdermal is always superior. This narrative is everywhere.
It’s also not true.
Oral estradiol absolutely has downsides. It undergoes first-pass liver metabolism, which means it stimulates the liver to produce more clotting factors. It can increase triglycerides. For women with certain cardiovascular risk factors, these effects matter and transdermal is genuinely the better choice.
But oral estradiol also has significant advantages that nobody talks about. It produces bigger drops in LDL cholesterol and ApoB. It increases HDL more effectively. It’s one of the few interventions that can meaningfully reduce Lp(a), which is notoriously difficult to treat. And here’s the kicker: most of the randomized cardiovascular outcome data we have in younger menopausal women comes from oral estrogen, not transdermal. The reassuring safety data? That’s oral estrogen.
Think of oral versus transdermal as different tools with different effects, not as good versus bad. If you have a history of clotting disorders or significantly elevated triglycerides, transdermal makes sense. If your primary concern is cardiovascular risk and you want the metabolic benefits, oral might actually be the better choice. This isn’t one-size-fits-all medicine, and pretending oral estradiol is categorically inferior does women a disservice.
9. Estradiol Helps Joint Pain (One of Its Best Hidden Perks)
This is one of my favorite things about estradiol and is the thing I noticed first when I started taking estrogen – my joint pain improved markedly!
Many women find that their aching hands, stiff knees, or morning stiffness improve shortly after starting estradiol, sometimes even before their hot flashes disappear. They wake up and realize they’re not shuffling around like the Tin Man anymore. Their hands don’t hurt when they open jars. Their knees don’t ache going up stairs.
Estradiol modulates inflammation, supports cartilage metabolism, and affects pain signaling pathways. Joint pain in perimenopause and menopause isn’t just about aging – it’s about losing a hormone that was keeping inflammation in check and supporting joint health. When you replace that hormone, the joints often respond.
Hallelujah!
10. Consistency Beats Creativity
Estradiol is a slow, steady hormone. It’s not like taking ibuprofen, where you feel different two hours later. It works by maintaining stable levels that allow your tissues to function as intended.
If you want reliable results, you need to keep a few things consistent:
Your application time. Roughly the same time each day matters more than you think. Estradiol levels fluctuate naturally without adding unnecessary variability.
Your application site category. You don’t need to hit the exact same square centimeter of skin every day, but bouncing between ten completely random spots (inner arm one day, outer thigh the next, abdomen the day after) introduces unnecessary inconsistency. Pick a category (forearms, thighs, lower abdomen) and stick with it.
Your dosing schedule. If you’re on a patch, change it on the same days. If you’re on a gel or cream, don’t skip days because you forgot or didn’t feel like it. Estradiol doesn’t work in bursts. It works with consistency.
Your levels and symptoms stabilize more effectively when your routine is routine. This is not the place to get creative. Save your spontaneity for literally anything else in your life.
11. If Your Estradiol Levels Look “Good” but You Don’t Feel Good, You’re Not Crazy
Here’s one of the most important things I can tell you: two women with the exact same serum estradiol level can feel completely different.
One woman might have an estradiol of 80 pg/mL and feel amazing. Another might have 80 pg/mL and feel like absolute garbage. Why? Estradiol’s effectiveness depends on much more than just the number on your lab report.
Stress affects how your body uses estradiol. Sleep quality matters. Thyroid function matters. Cortisol levels matter. Insulin sensitivity matters. Local tissue responsiveness to estrogen (which we can’t easily measure) matters enormously. Even the balance between estradiol and progesterone or testosterone can shift how you feel, independent of the estradiol level itself.
If your labs come back “fine” but you feel terrible, that doesn’t mean the treatment is wrong. It doesn’t mean you’re imagining things. It doesn’t mean your doctor should shrug and tell you this is as good as it gets. It means we should look at the route of administration, consider adjusting the dose, evaluate absorption issues, and examine the whole-body context that determines whether estradiol can actually do its job.
Symptoms always matter. You are not a lab value. You are a person who deserves to feel well, and if something isn’t working, that merits investigation, not dismissal.
Final Thought
Estradiol isn’t magic… But it’s damn near close!
And when women understand how to use it (not just that they can use it), outcomes improve dramatically.
You deserve to know this stuff. You deserve to feel good. And you deserve doctors who understand that optimizing hormone therapy is an art as much as a science.
If you found this helpful, share it with someone who might need it. The more women who know how to actually use their HOT effectively, the fewer women suffer needlessly.
And if you’re not on hormone therapy yet but think you might benefit, print this out and bring it to your next appointment. Knowledge is power, and it’s time you took back yours.
References:
Estradiol gels, surface area, and transdermal PK
-
Ojala K, Sarvilinna N, Männistö T, Ylikorkala O. Steady-state pharmacokinetics of oestradiol gel in post-menopausal women. Maturitas. 1997;28(2):155‑162.
-
O’Sullivan AJ, et al. Comparative absorption and variability in absorption of estradiol from a transdermal gel and a matrix-type transdermal patch. J Clin Pharmacol. 2001;41(11):1291‑1297.
-
Medsafe. Estrogel (estradiol gel) Data Sheet. [Product information].
Oral vs transdermal estradiol: lipids, Lp(a), coagulation, CVD markers
-
Vehkavaara S, et al. Differential effects of oral and transdermal estrogen replacement therapy on endothelial function in postmenopausal women. Circulation. 2000;102(22):2687‑2693.
-
Scarabin P-Y, et al. Effects of oral and transdermal estrogen replacement therapy on hemostasis variables and inflammatory markers. Thromb Haemost. 2003;89(3):460‑467.
-
Mikkola TS, et al. Differing effects of oral and transdermal hormone replacement therapy on cardiovascular risk factors in healthy postmenopausal women. Menopause. 2003;10(6):550‑557.
-
Santen RJ, et al. Menopausal hormone therapy and cardiovascular disease: the role of formulation, dose, and route of delivery. J Clin Endocrinol Metab. 2021;106(5):e1960‑e1974.
Vaginal estrogen and systemic estradiol levels
-
Santen RJ, et al. Systemic estradiol levels with low-dose vaginal estrogens. Menopause. 2020;27(3):361‑370.
-
Crandall CJ, et al. Association of vaginal estradiol tablet with serum estrogen levels in women who are postmenopausal: secondary analysis of a randomized clinical trial. JAMA Netw Open. 2022;5(11):e2241825.
-
Simon JA, et al. Systemic effects of vaginally administered estrogen therapy: a review. J Womens Health (Larchmt). 2005;14(12):1093‑1102.
Joint pain and musculoskeletal symptoms
-
Chlebowski RT, et al. Estrogen alone and joint symptoms in the Women’s Health Initiative randomized trial. Menopause. 2013;20(6):600‑608.
-
The WHI investigators. Estrogen-alone trial primary reports and subsequent musculoskeletal secondary analyses (reviewed in: Reappraising 21 years of the WHI study. Maturitas. 2023).
Guidelines and higher-level summaries
-
The North American Menopause Society. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. 2022;29(7):767‑794.
-
ACOG Clinical Consensus. Treatment of urogenital symptoms in individuals with a history of estrogen-dependent breast cancer. Obstet Gynecol. 2021;138(6):950‑960. (Covers systemic levels and safety framing for vaginal estrogen.)
This article was originally published on Dr. Amy Killen’s Substack newsletter. Subscribe for free to get new posts delivered to your inbox.
Are you a medical provider? Learn to prescribe hormone optimization therapy with the frameworks, protocols, and confidence you didn’t get in training.
Get Dr. Amy Killen’s Newsletter
Hormones, longevity, and regenerative medicine — straight talk from a physician who actually prescribes it. Free, weekly-ish, no spam.