Why has your body stopped making enough
Meet Sarah (She’s All of Us)
Sarah is 42. For most of her adult life, her periods showed up like clockwork, she slept like a normal human, and the week before her period was… fine. Maybe she wanted more chocolate than usual, but who doesn’t?
Then, about a year ago, everything changed. Two weeks before her period, she started waking up at 3 AM with her heart racing and a sense of impending doom that felt completely irrational but also very real. She’d lie there spiraling about whether she remembered to pay the electric bill, if her kid’s teacher hates her, and why she said that weird thing at the work meeting three years ago.
She went to her doctor. The doctor, a perfectly nice man who definitely doesn’t have a menstrual cycle, prescribed Ambien and jokingly said, “Now don’t go buying an alpaca farm on Ambien at 3 AM, ya hear??”
Cool. Cool. So Sarah’s hormones are changing, her body is trying to tell her something, and the solution is… sleeping pills and a warning about online shopping sprees?
Here’s what Sarah’s doctor missed: her progesterone was tanking.
And Sarah is not alone. This is the story of basically every woman in her 40s (and plenty in their 30s too) who suddenly feels like she’s losing her grip on her sanity for two weeks out of every month.
Why Would a Cycling Woman Need Extra Progesterone Anyway?
If your ovaries are supposed to be making progesterone every month after ovulation, why would you need to supplement it? Let’s talk about five reasons your progesterone might be running low, even if you’re nowhere near menopause.
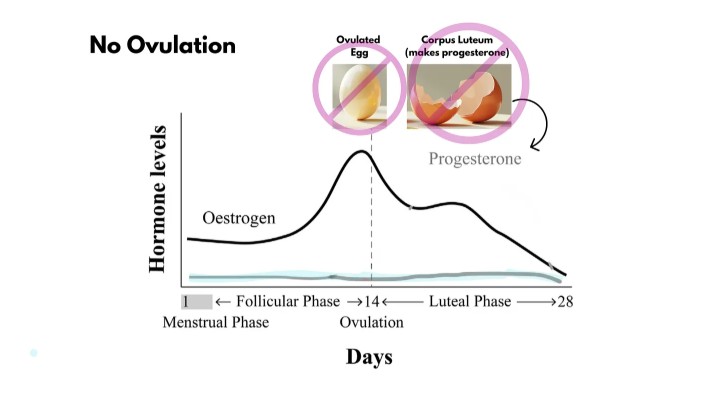
The Root Cause: You’re Not Ovulating (Or Not Ovulating Well)
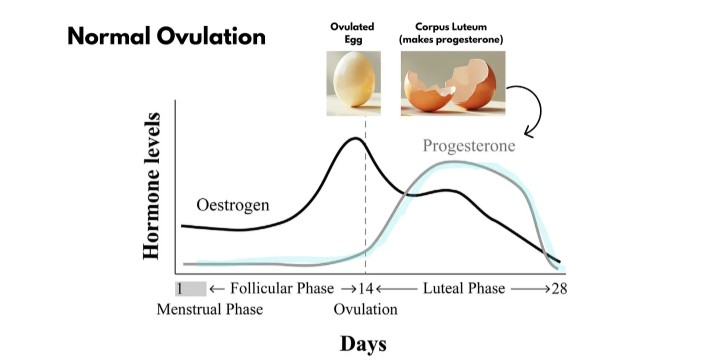
Progesterone comes from the corpus luteum, which is that little hormone-making shell that surrounds the egg that forms after you ovulate. No ovulation? No corpus luteum. No corpus luteum? No progesterone. It’s that simple.
However, anovulation (not ovulating) doesn’t occur randomly. Something is causing it. You may be having cycles where you bleed but rarely release an egg. Or maybe you ovulate but your corpus luteum is weak and doesn’t produce enough progesterone, like an engine sputtering along on half power. Either way, the result is the same: not enough progesterone to make you feel human.
What causes anovulation or weak ovulation? There are several overlapping culprits…
Cause #1: Thyroid Dysfunction (Your Thyroid and Ovaries Are Frenemies)
Your thyroid and your ovaries are deeply interconnected. When one struggles, the other does too.
Hypothyroidism (underactive thyroid) messes with ovulation in multiple ways. First, it disrupts your entire endocrine system, making it more difficult for your ovaries to function correctly. Second, a peculiar bidirectional phenomenon is occurring: low progesterone reduces the availability of free thyroid hormone to your cells (as progesterone affects thyroid-binding proteins), and low thyroid hormone hinders the production of progesterone. It’s a vicious cycle where each one makes the other worse.
Even hyperthyroidism (overactive thyroid) can tank your progesterone through increased oxidative stress that damages ovarian function. Your thyroid needs to be in the Goldilocks zone for your ovaries to produce adequate progesterone.
If you’ve got thyroid issues (especially Hashimoto’s or hypothyroidism) and you’re also dealing with progesterone-related symptoms, this is probably why. Fix the thyroid, and the progesterone often improves. Ignore the thyroid, and you’re just spinning your wheels.
Cause #2: Chronic Stress (Your Brain Pulls the Emergency Brake)
You’ve probably heard about “pregnenolone steal” – the idea that stress steals your progesterone to make cortisol. That theory has been debunked. Your adrenals don’t actually steal progesterone; they make their own hormones independently in different zones that don’t share resources.
But stress absolutely does tank your progesterone – just not through stealing. Here’s the real mechanism: when your brain perceives chronic stress (work, relationships, financial pressure, overtraining at the gym, doing All The Things), your hypothalamus, the control center upstairs, shuts down your reproductive system. It downregulates the hormones (FSH and LH) that tell your ovaries to ovulate.
Think of it like your brain saying, “This is NOT a good time to make a baby, so we’re closing the baby factory until further notice.” No ovulation means no progesterone. It’s not a resource problem; it’s a priority problem.
Interestingly, acute stress (like a workout) actually increases both cortisol and progesterone temporarily. But chronic, unrelenting stress? This disrupts ovulation through a condition known as HPA axis dysfunction, resulting in anovulatory cycles and progressively lower progesterone levels. Add in the fact that chronic stress also causes insulin resistance and inflammation (which further impair ovarian function), and you’ve got a multi-layered hormonal disaster.
Cause #3: Insulin Resistance and Metabolic Dysfunction (The Hidden Epidemic)
This is the big one that nobody talks about enough. Insulin resistance affects 20-30% of cycling women and is a massive driver of low progesterone in women who don’t even know they have metabolic issues.
Here’s how it works: when your cells become resistant to insulin (from too much sugar, refined carbs, stress, lack of sleep, etc.), your insulin levels stay chronically elevated. High insulin interferes with normal follicle development in your ovaries and disrupts ovulation. No proper ovulation? No adequate progesterone.
But it gets worse. Low progesterone leads to “estrogen dominance,” which worsens insulin resistance. So you end up in a vicious cycle: insulin resistance → anovulation → low progesterone → estrogen dominance → worse insulin resistance. Round and round you go.
Note: “Estrogen dominance” isn’t a real medical term, but it’s an easy way to explain that the estrogen to progesterone ratio is higher than ideal and that wonky up ratio is now causing symptoms.
Research shows that insulin is one of the primary hormones that needs to be balanced before other hormones (like progesterone) can normalize. You can supplement all the progesterone in the world, but if you don’t address the underlying insulin resistance, you’re just putting a band-aid on a bullet wound.
This is why things like cutting back on sugar and refined carbs, improving sleep, managing stress, and engaging in regular physical activity can have such a profound effect on progesterone levels – you’re addressing the metabolic dysfunction driving the whole problem.
Cause #4: PCOS (Where Everything Converges)
PCOS (polycystic ovary syndrome) isn’t just one thing – it’s where multiple causes crash into each other like a hormonal pile-up on the freeway. Women with PCOS often have:
- Anovulation (the immediate cause of low progesterone)
- Insulin resistance (driving the metabolic dysfunction)
- High androgens like testosterone (disrupting normal follicle development)
- Chronic inflammation (perpetuating the whole mess)
PCOS actually overstimulates the immune system, leading to increased inflammation and even the production of autoantibodies. So it’s not just that PCOS causes low progesterone – low progesterone makes PCOS worse by ramping up inflammation.
If you have PCOS, supplementing progesterone can help manage symptoms and protect your uterine lining, but you also need to address the root causes; otherwise, you’re just managing symptoms without fixing the underlying problem.

Cause #5: High Prolactin (The Breastfeeding Hormone That Overstays Its Welcome)
Prolactin is the hormone that’s supposed to be high when you’re breastfeeding. it helps produce milk and temporarily shuts down ovulation (nature’s way of spacing out pregnancies). But sometimes prolactin stays elevated when you’re not breastfeeding, and that’s a problem.
Elevated prolactin (hyperprolactinemia) directly suppresses your ovaries’ production of estrogen and progesterone. It creates what’s called a “luteal phase defect,” where even if you ovulate, your corpus luteum is weak and doesn’t produce enough progesterone. It also impairs LH (luteinizing hormone), which is necessary for forming a healthy corpus luteum in the first place.
High prolactin can be caused by certain medications (especially antidepressants and antipsychotics), thyroid problems, pituitary tumors (usually benign), or chronic stress. If you’re having symptoms of low progesterone plus things like irregular periods, breast milk production when you’re not nursing, or low libido, it’s worth checking your prolactin levels.
Cause #6: When Your Ovaries Start Fizzling Out
All of the above can happen at any age. But for women in their 40s (and sometimes late 30s), there’s one more massive reason for low progesterone: your ovaries are winding down.
This is what’s happening to Sarah.
As you approach menopause, your ovaries start to run out of eggs (you’re born with all you’ll ever have), and the eggs you have left are older and less responsive. Ovulation becomes less frequent and less robust. Even when you do ovulate, your corpus luteum might be wimpy and produce less progesterone than it used to – like a dying flashlight that’s flickering instead of shining bright.
Progesterone production drops FIRST, way before estrogen. Sometimes, years before your periods actually stop.
Meanwhile, estrogen production often holds steady or even increases in early perimenopause. Sometimes estrogen levels surge higher than they’ve been in years (thanks to your brain frantically pumping out more FSH trying to get your stubborn ovaries to ovulate). This is why some women get absolutely steamrolled by worse PMS, heavier periods, and new symptoms in their 40s, even though they were fine in their 30s.
So you end up with “estrogen dominance,” not because estrogen is sky-high (although it can be), but because progesterone has left the building and estrogen is sitting there unopposed, like a toddler with no supervision and a Sharpie.
This is what’s happening to Sarah. Her progesterone is dropping, her estrogen is still showing up for work, and the ratio between them is completely out of whack. The result?
- Anxiety that shows up like clockwork in the luteal phase
- Insomnia (especially that fun 3 AM wake-up where your brain decides to replay every embarrassing thing you’ve ever done)
- Premenstrual migraines
- Periods that are heavier, longer, or more painful
- Breast tenderness that makes you want to wear a sports bra to bed
- Brain fog that makes you forget why you walked into a room
- Weight gain around the middle that seems to appear overnight
- The overwhelming urge to murder everyone around you for minor infractions
And instead of progesterone, Sarah got Ambien and a dad joke.
The good news? Once you understand why your progesterone is low, you can actually do something about it. And that’s where cycling progesterone comes in.
Coming Next Week: Part II – Cycling Progesterone in Women: Finding Your Rhythm without Losing Your Mind
In Part II, we’ll dive into the how. I’ll walk you through the four most common ways to cycle progesterone if you’re still having regular (or regular-ish) periods. We’ll discuss how to work in harmony with your body’s rhythm instead of against it.
Plus, I’ll explain what happens when you don’t cycle progesterone and instead take the same dose every day. Spoiler: for some women, it’s fine, but for others, it turns a predictable cycle into a complete mystery.
See you then. And in the meantime, maybe get your thyroid checked. Just saying.